Domiciliary, Rest Home, or Custodial Care Services CPT codes 99324 - 99337
These codes are also used to report E/M services in an assisted living facility. The facility’s services do not include a medical component.
A home or domiciliary visit includes a patient History, Physical Examination and Medical Decision Making in various levels depending upon a patient’s needs and diagnosis.
The visits may also be performed as counseling and/or coordination of car, when medically necessary outside the office environment and are an integral part of a continuous of the patient's care.
The patients seen may have chronic conditions, may be disabled, either physically or mentally, making access to a traditional office visit very difficult, or may have limited support systems.
The home or domiciliary visit in turn can lead to improved medical care by identification of unmet needs, coordination of treatment with appropriate referrals and potential reduction of acute exacerbation of medical conditions, resulting in less frequent trips to the Hospital or Emergency services.
The home-based health care is rapidly expanding and growth in hospital-based house call programs.
The Physicians and qualified non-physician practitioners (NPPs) are required to oversee or directly provide progressively more involving a great deal of worldly experience and knowledge of fashion and culture for home visits.
A Patients must understand the nature of a pre-arranged visit and consent to treatment in the home or domiciliary care facility. There is no requirement that the patient must be homebound.
If the service is provided to a patient for the first time, the patient, his/her delegate, or another medical provider managing the patient’s care, must request the service. The visiting provider may not directly solicit referrals.
- An example of inappropriate solicitation is knocking on residents’ doors or placing calls to residents on the telephone to offer medical care services when there has been no referral from another professional that is already involved in the case.
If laboratory and diagnostic tests are performed during the course of home or domiciliary care visits, they must be documented in the medically necessary reason. Medical reasons for repeat testing must be clearly documented.
Every page of the record must be legible and include appropriate patient identification information (e.g., complete name, dates of service[s]).
The documentation must include the legible signature of the physician or non-physician practitioner responsible for and providing the care to the patient.
Many elderly patients have chronic conditions, such as hypertension, diabetes, orthopedic conditions, and abnormalities of the toenails.
Required Criteria
- A home or domiciliary care visit must meet all of the following criteria.
- Chief complaint or a specific, reasonable, and medical necessity is required for each visit.
- A payable diagnosis alone does not support medical necessity of ANY service.
- Medical necessity must exist for each individual visit.
- Visit will be regarded as a social visit unless medical record clearly documents medical necessity for every visit.
- Service/visit must be medically reasonable and necessary and not for physician or qualified NPP convenience.
- Service must be of equal quality to a similar service provided in an office.
- Frequency of visits required to address any given clinical problem should be dictated by medical necessity rather than site of service.
- It is expected that frequency of visits for any given medical problem addressed in home setting will not exceed that of an office setting, except on rare occasion.
- Training of domiciliary staff is not considered medically necessary.
- The E/M service will not be considered medically necessary when it is performed only to provide supervision for a visiting nurse/home health agency visit(s).
Acceptable Location
Home based services are provided services which are performed in,
- Private Residence - Home, apartment, town-home etc.
- Domiciliary Care Facility - A home providing mainly custodial and personal care for persons who do not require medical or nursing supervision, but may require assistance with activities of daily living because of a physical or mental disability. This may also be referred to as a sheltered living environment.
- Rest Home - A place where people live and are cared for when they cannot take care of themselves.
- Custodial Care Services - Custodial care is non-medical assistance, either at home or in a nursing or assisted-living facility with the activities of daily life (such as bathing, eating, dressing, using the toilet) for someone who's unable to fully perform those activities without help.
- Residential Substance Abuse Facility - A facility which provides treatment for substance (alcohol and drug) abuse to live-in residents.
Place of Service (POS) Codes
- 12 - Home
- 13 - Assisted Living Facility (adult living facility)
- 14 - Group Home
- 33 - Custodial Care Facility
- 55 - Residential Substance Abuse Facility
Domiciliary, Rest Home, or Custodial Care Services Listing -CPT 99324 to 99337
CPT Code Description
99324 Level 1 new patient domiciliary, rest home, or custodial care visit
99325 Level 2 new patient domiciliary, rest home, or custodial care visit
99326 Level 3 new patient domiciliary, rest home, or custodial care visit
99327 Level 4 new patient domiciliary, rest home, or custodial care visit
99328 Level 5 new patient domiciliary, rest home, or custodial care visit
99334 Level 1 established patient domiciliary, rest home, or custodial care visit
99335 Level 2 established patient domiciliary, rest home, or custodial care visit
99336 Level 3 established patient domiciliary, rest home, or custodial care visit
99337 Level 4 established patient domiciliary, rest home, or custodial care visit
Home Visits Listing - CPT codes 99341 - 99350
- The Home Services codes, are used to report E/M services furnished to a patient residing in his or her own private residence.
- The Private residence considered following, Private home, an apartment, or town home.
CPT Code Description
99341 Level 1 new patient home visit
99342 Level 2 new patient home visit
99343 Level 3 new patient home visit
99344 Level 4 new patient home visit
99345 Level 5 new patient home visit
99347 Level 1 established patient home visit
99348 Level 2 established patient home visit
99349 Level 3 established patient home visit
99350 Level 4 established patient home visit
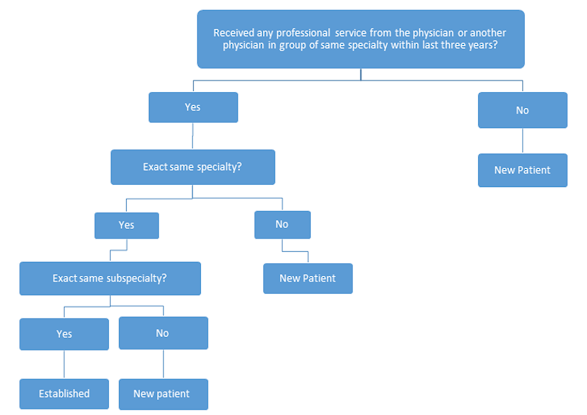
Refer New Patient vs. Established Guidelines